The Aortic Adverse Event Report
A consult report patients can follow — year by year
For physician consultation only. Not intended as medical advice for individual patients.
Sample report — de-identified · generated at the point of care · no EMR required
A Standardized Report, Not a Guess
Three surgeons, three different risk estimates — with no way to reconcile them. That's the experience most patients facing an aortic aneurysm actually have. It's a delivery failure, not a scientific one: the underlying evidence is well established, but its application varies by physician.
The Aortic Adverse Event Report fixes that. It applies the same evidence-based methodology to every patient, producing the same result regardless of which physician generates it — a standardized, timestamped, physician-authored record the patient can hold onto and revisit.
Makes the Risk Personal
A year-by-year trajectory, not a single abstract percentage — patients who see their own data commit to timely follow-up.
Same Report, Every Institution
Standardized methodology means a second opinion yields the same number — so patients trust the data enough to act on it.
No EMR Needed
Secure web portal, any device. A permanent report is generated immediately and can be shared, stored, and tracked over time.
Grounded in Published Evidence
Built on Elefteriades/Davies natural history data, the IRAD registry, and ACC/AHA 2022 guideline thresholds.
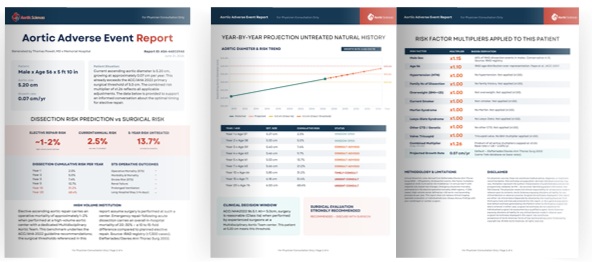
Why a 30-Year Projection Changes the Conversation
A 3% annual dissection risk is abstract. Projected forward — accounting for continued aortic growth of approximately 0.07 cm/year (Elefteriades/Davies) and the resulting progression through higher-risk diameter brackets — the cumulative picture becomes both more accurate and more actionable.
A patient today at 4.8 cm with hypertension and BAV does not face a static annual risk. Over the next decade, as that aorta grows, annual event probability climbs into successively higher brackets. The 10-year cumulative risk may be multiples of today's estimate — making watchful waiting appear far less conservative than the current snapshot suggests. A year-by-year trajectory transforms an abstract percentage into a concrete decision support tool.
Elective vs. Emergency: A 10–20x Mortality Difference
Acute Type A aortic dissection carries a 30-day operative mortality of 21–25% at experienced centers, per IRAD data across 7,300+ cases. Elective ascending aortic repair at those same centers: 1–2%. That gap — 10 to 20 times — is the central argument for timely, individualized risk assessment.
The window between surveillance and surgery is where outcome is determined. A patient converted from watchful waiting to planned elective repair faces a fundamentally different risk profile than the same patient who presents in dissection. ACC/AHA 2022 guidelines encode this logic into intervention thresholds — but thresholds alone don't account for the full individual risk picture.
Beyond Diameter Alone
Aortic size is the starting point, not the full picture. The report layers in the patient's individual risk factors — valve anatomy, connective tissue and genetic history, family history of dissection, hypertension, root involvement, aortic length, age, and sex — using a multiplicative risk model built on published literature and refined with our Advisory Board of leading aortic surgeons.
The specific weighting behind each factor is proprietary to Aortic Sciences and detailed in full for participating physicians and institutions. What patients and referring physicians see is the output: a clear, individualized, year-by-year risk trajectory built on that evidence base — not a diameter measurement in isolation.
Bring the Aortic Adverse Event Report to Your Program
Schedule a 20-minute demo of the Aortic Sciences physician portal — secure, browser-based, no EMR required.
For physician consultation only. Not intended as medical advice for individual patients. Aortic Sciences.